News and Blog
NHSE seeks department views on resuming training of AAs

Current RCoA policy is that there should be no new recruitment of student Anaesthesia Associates. But NHSEngland is hoping to resume recruitment of student AAs in London in the future.
They are looking for Anaesthetic Departments in the London ICS that may be interested, and are shortly to survey individual departments. The clinical lead (or deputy) will be asked to reply on behalf of their colleagues, and it is the intention that the overall views of the full department are reflected.
It would seem wise for departments to discuss amongst themselves their attitudes and interest in taking part in this proposed expansion.
It could be Game Over for national recruitment, following Department of Business and Trade decision

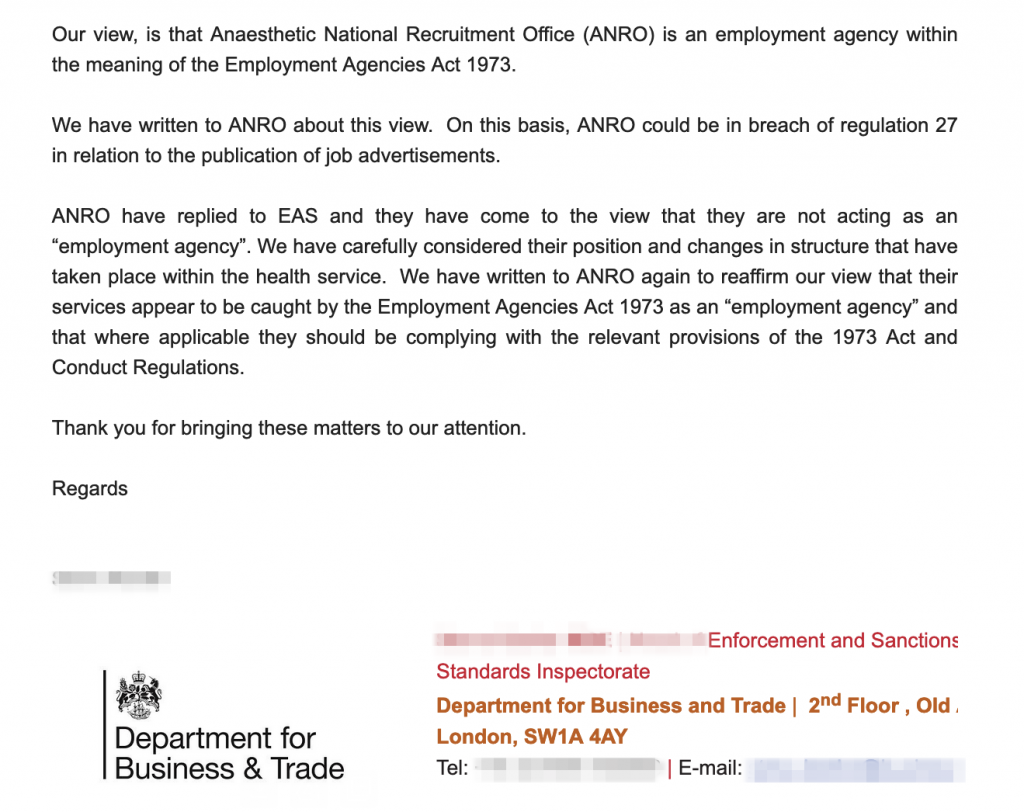
After over 6 months of legal delay following our initial report, the Head of Enforcement and Sanctions at the Department of Trade has delivered a verdict. The Anaesthetic National Recruitment Office (ANRO) is an Employment Agency (EA) within the meaning of the 1973 Act … and could be in breach of regulation 27. This verdict will have profound implications for workers rights.
Although ANRO does not fit the typical picture of an EA the legal definition of an Agency is very wide and extensive, and encompasses many other professional sectors.
This decision means that there are liabilities, duties and responsibilities for ANRO which, even with the best will in the world, may be impossible for them to achievable. It may no longer be feasible to continue with national recruitment in its present form.
Employment Agencies have civil liability. Contravention of any of the provisions of the Act by an Agency can lead to a claim for damages. This could include, for example, any financial costs incurred if a rotation is unexpectedly changed or announced late. Employment Agencies can also be subject to fines and prosecution for breaches, especially when these are persistent.
There is also, at last, some accountability for individuals. Where an offence under this Act … is proved to have been committed with the consent or connivance of … any director or a person who was purporting to act in any such capacity, he, as well as the body corporate, shall be guilty of the offence and shall be liable to be proceeded against and punished accordingly.
As a brief aside, the “Lead Employer” model is not directly relevant to this issue, unless the employer directly carries out the recruitment themselves.
ANRO themselves, however, do not accept the Employment Agency Standards Inspectorate (EASI) opinion. No explanation for this has been given. Presumably it is an inconvenient truth that they would prefer to go away. Maybe ANRO doesn’t listen to experts.
The government could attempt to amend the relevant legislation, as a previous government unsuccessfully tried in 2009, but first there is a statutory requirement for consultation, together with the need to establish under what other possible legal basis ANRO could be acting as recruiter for Trust jobs.
Over the next few weeks our legal advisors will be looking at both individual and class actions that are possible in the light of this decision.
The letter from EASI
Information given to applicants within 3 days of an offer
Employment Agencies must give workers detailed information regarding
- Their exact pay, and details of both deductions and travel expenses,
- The location and hours of work, and
- Any health and safety risks and the steps in place to reduce these risks.
This information must be given no later than 3 days after making a job offer.
The employers themselves should receive details of the work-seeker within the same 3 day period, including two references. There are specific requirements on wording of advertisements.
If these requirements are not met, then agencies may be subject to enforcement action, such as fines or other penalties.
Pre-employment checks must be carried out by the Agency
Carrying out checks such as passports, DRB and academic qualifications, a process endlessly repeated under rotational training, is the responsibility of the Employment Agency and not of the employer. There are obvious good fiscal and logistic reasons for this as well, regardless of the law.
Separation of recruitment from other activities
Perhaps the biggest consequence is that NHSE_WTE may not legally or practically be able to carry out both the recruitment and the other educational and supervisory functions it fulfils. Partly because an EA cannot disclose information relating to a work-seeker to the employer except under very specific circumstances. And partly because they are expressly prohibited from requiring a work-seeker to use any of their other services.
No minimum period of notice to the Agency
It is unlawful to submit a work-seeker to any detriment on the ground that the work-seeker has terminated or given notice to terminate their contract with an Agency (though be aware that employment contracts with Trusts, often fixed-term, are managed differently). Agencies do not have to be told where you are going when you leave.
Holiday pay
Agency workers and employees have the right to carry over periods of holiday not taken to a new assignment, and can expect to get paid for any holiday they haven’t taken when they leave.
Other specialties and Foundation Training
Other recruitment offices run by NHSE_WTE (formerly HEE) are likely to be implicated in this decision since they function in a similar way to ANRO. Some of these, including those covering Foundation, General Practice and Psychiatry, have already announced in their Terms of Business that they are awaiting this decision and will adhere to the law.
Further reading and references
Government overview of Employment Agencies
https://www.gov.uk/employment-agencies-and-businesses
Employment Agency Standards Inspectorate – A brief guide for agencies
ACAS – Agency worker – your employment rights
https://www.acas.org.uk/agency-workers/understanding-your-employment-rights-as-an-agency-worker
The Conduct of Employment Agencies and Employment Businesses Regulations 2003
https://www.legislation.gov.uk/uksi/2003/3319/contents/made
Employment Agencies Act 1973
https://www.legislation.gov.uk/ukpga/1973/35/contents
Make a complaint about an Employment Agency
If you want to make a complaint about
- Breaches of your privacy
- Delay in receiving the correct information (which may have had a financial impact), or
- Any of the other issues listed above
you can do this online at https://www.gov.uk/government/publications/pay-and-work-rights-complaints
You will need the address and postcode of the agency which is easy to find.
If you are affected by this and wish to contact us then please send emails to agencies@schoolofanaesthesia.co.uk
Ensuring that persons providing care have the qualifications and skills

There has been a lot of talk lately about safe care and treatment. In particular, whether or not Associates and non-doctors have the qualifications, competence, skills and experience to deliver treatment safely. But there’s also some uncertainty over which of the many organisations involved in protecting the public are responsible for assessing and enforcing this … Read more
RCoA EGM on 17th October – the Recruitment Motions

On 17th October the Royal College of Anaesthetists is holding an Extraordinary General Meeting. The EGM was called for by Anaesthetists United, a group that I am closely involved with. Much of the interest has revolved around Anaesthesia Assistants and this has become a mainstream issue in the national press. But there are two other … Read more
ANRO under investigation by Dept of Business and Trade over workers rights

The Enforcement and Sanctions office at the Department of Business and Trade has agreed to investigate whether ANRO – the Anaesthetic National Recruitment Office – is complying with regulation 27 of the 2003 Employment Agencies (EA) Act. They have agreed that … based on the information available, it would appear that ANRO’s services might be … Read more
Older News....
July 2023
The mistakes in Anaesthetics Recruitment in 2021 – where did it go wrong?Time to end the August changeover chaos